Imagine waking up, rolling over to check your phone, and suddenly the entire room starts spinning like a carousel. You aren't moving, but your brain is convinced you are. This unsettling sensation is exactly what happens during an episode of vertigo. While many people use "dizziness" as a catch-all term, there is a massive difference between feeling lightheaded and experiencing the spinning sensation of true vertigo. For some, it's a brief 20-second blur; for others, it's a debilitating condition that makes walking in a straight line feel like a dare. The good news? Most of these issues stem from the inner ear and are highly treatable once you stop guessing and start testing.
Quick Summary of Key Takeaways
- Vertigo vs. Dizziness: Vertigo is a spinning sensation; dizziness is general lightheadedness.
- Main Cause: About 80% of cases are peripheral, meaning they start in the inner ear.
- BPPV: The most common cause, often fixed quickly with a specific head maneuver.
- Treatment: Vestibular therapy helps the brain compensate for balance loss through neuroplasticity.
- Red Flag: Acute prolonged vertigo requires a stroke evaluation within 48 hours.
The Science of the Spin: What is Actually Happening?
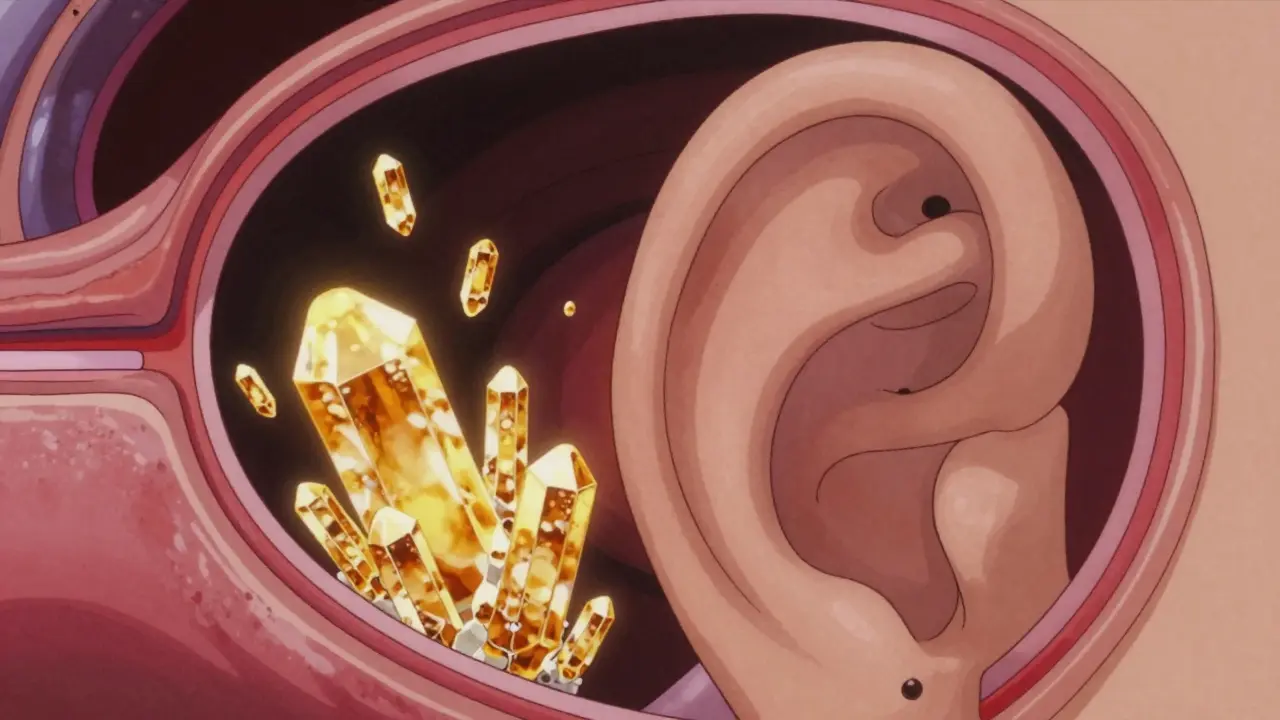
To understand why you feel like the world is tilting, you have to look at the Vestibular System. This is the sensory system in your inner ear that provides your brain with a sense of balance and spatial orientation. When this system sends conflicting signals to your brain-telling it you're spinning when you're actually still-you experience Vertigo, which is a sensation of movement or spinning when no actual motion is occurring.
Medical experts divide these issues into two camps: peripheral and central. Peripheral Vertigo accounts for roughly 80% of cases and happens when something goes wrong in the inner ear or the vestibulocochlear nerve. On the flip side, central vertigo involves the brainstem or cerebellum. While less common, central causes like Vestibular Migraine can affect up to 3% of the population and often last much longer-anywhere from a few minutes to 72 hours.
Common Inner Ear Culprits
Not all vertigo is created equal. Depending on the cause, your symptoms will look very different. The most frequent offender is Benign Paroxysmal Positional Vertigo (or BPPV), which is a disorder where tiny calcium carbonate crystals, called otoconia, dislodge and float into the semicircular canals of the inner ear. This triggers short, intense bursts of spinning-usually lasting 5 to 30 seconds-whenever you tilt your head back or roll over in bed.
Then there is Meniere's Disease. Unlike the quick hits of BPPV, this involves a buildup of fluid (endolymphatic hydrops) in the inner ear. If you have this, you'll likely notice attacks lasting from 20 minutes up to a full day, accompanied by a "full" feeling in your ear, ringing (tinnitus), and fluctuating hearing loss. It's a more complex condition that usually requires a combination of diet and medication.
Lastly, some people deal with Vestibular Neuritis. This is typically caused by a viral infection that inflames the vestibular nerve. It creates a prolonged period of spontaneous vertigo that can last for days or weeks, though interestingly, it usually doesn't affect your hearing.
| Condition | Primary Cause | Duration of Episode | Key Accompanying Symptoms |
|---|---|---|---|
| BPPV | Displaced crystals (otoconia) | 5-30 seconds | Triggered by head movement |
| Meniere's | Fluid buildup in inner ear | 20 mins - 24 hours | Hearing loss, Tinnitus |
| Vestibular Neuritis | Viral inflammation of nerve | Days to weeks | Severe nausea, no hearing loss |
| Vestibular Migraine | Central nervous system/Migraine | Minutes to 72 hours | Sensitivity to light/sound |
How to Stop the Spinning: Treatment Options
If you have BPPV, you don't need long-term medication; you need a physical correction. The Epley Maneuver is the gold standard here. By moving your head through a specific sequence of positions, a therapist can essentially "dump" those loose crystals back where they belong. Statistics show this is effective in 80-90% of cases after just a few sessions. In fact, some patients report their world stopping its spin in under 15 minutes.
For those with Meniere's, the focus shifts to fluid management. This often means taking a diuretic (water pill) and sticking to a strict sodium limit of 1,500 to 2,000mg per day. Since most of our salt comes from processed foods, this is often the hardest part of the treatment. However, those who stick to the diet often see a 50-70% reduction in the frequency of their attacks.
When it comes to meds, people often reach for Meclizine. While it's great for stopping nausea during an acute attack, using it for too long is actually a mistake. If you stay on vestibular suppressants for more than 72 hours, you might actually delay your recovery by 30-50% because your brain stops trying to fix the problem on its own.
Reclaiming Your Balance with Vestibular Therapy
When the initial attack fades but you're still feeling "off" or unsteady, it's time for vestibular therapy. This isn't just gentle stretching; it's a targeted exercise program designed to use your brain's neuroplasticity to compensate for a damaged inner ear. If one ear isn't sending the right signals, the brain can be trained to rely more on the other ear and your vision to keep you upright.
A typical program lasts 6 to 8 weeks and involves a few key techniques:
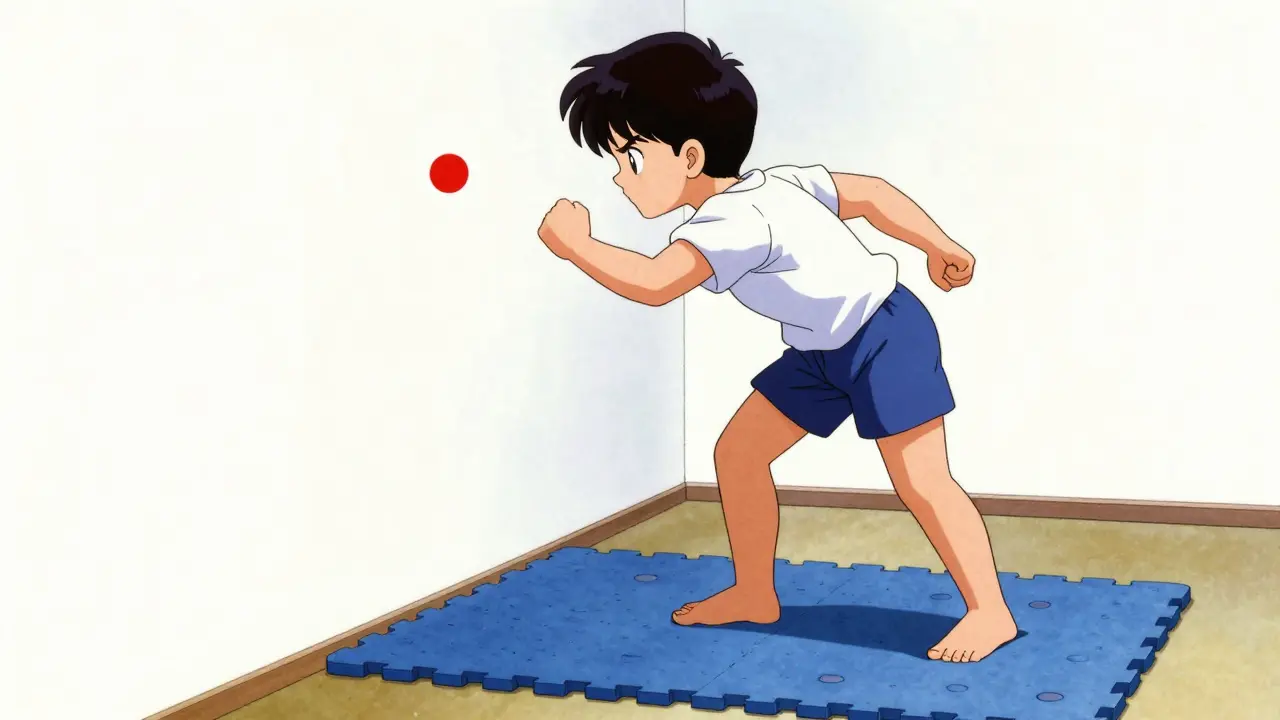
- Gaze Stabilization: Exercises like the Brandt-Daroff method, where you move your head while focusing on a fixed point to stop the world from jumping.
- Balance Retraining: Standing on uneven surfaces (like a foam mat) to force the brain to use different sensory inputs.
- Habituation: Repeatedly performing the movements that make you dizzy until your brain gets bored of the signal and stops reacting with vertigo.
Be warned: the first two weeks of therapy can actually make you feel worse. About 40% of patients report increased dizziness initially. But the data is clear-95% of people who push past that initial hump and stay consistent for two weeks see meaningful improvement.
When to Worry: The Red Flags
Not all dizziness is a simple inner ear glitch. In some cases, vertigo is the first sign of a stroke or a serious neurological event. This is why the HINTS exam (Head Impulse, Nystagmus, Test of Skew) is so critical in emergency rooms. When performed within 48 hours of the first symptom, it can identify a stroke with nearly 97% sensitivity.
You should seek immediate emergency care if your vertigo is accompanied by:
- Sudden, severe headache
- Double vision or blurred vision
- Difficulty speaking (slurred speech)
- Numbness or weakness in the face or limbs
- Inability to walk or sudden loss of coordination
Can I do the Epley maneuver at home?
Yes, home-based maneuvers can be 70-80% effective, but they are tricky. You need a precise 30-degree head angle and specific pauses. If you do it wrong, you might move the crystals into a different canal, making the vertigo worse. It's best to have a professional guide you through the first few sessions.
Why did my doctor say my dizziness was just anxiety?
BPPV and other vestibular disorders are frequently misdiagnosed as anxiety or general dizziness because they aren't always obvious in a standard check-up. About 50% of BPPV cases are initially misdiagnosed because the doctor didn't perform a positional test like the Dix-Hallpike maneuver.
How long does vestibular rehabilitation take to work?
Most patients see significant improvement within 4 to 6 weeks of consistent practice. The key is adherence; you generally need to perform the exercises twice daily to see the best results.
Does a low-salt diet actually help with Meniere's?
Yes. Restricting sodium to 1,500-2,000mg daily helps reduce the fluid buildup in the inner ear (endolymphatic hydrops), which can reduce the frequency of vertigo attacks by 50-70% for many patients.
Are there any permanent cures for vertigo?
For BPPV, the Epley maneuver can provide an immediate and lasting resolution. For chronic conditions like Meniere's, the goal is management. However, advanced options like endoscopic vestibular neurectomy offer up to 90% vertigo control for those who don't respond to other treatments.
Next Steps for Recovery
If you're currently struggling with balance, your first move should be a visit to an ENT (Ear, Nose, and Throat specialist) or a neuro-otologist. Don't just tell them you're "dizzy"-be specific. Tell them if the room spins, if it only happens when you roll over in bed, or if you have a ringing in your ears. This helps them choose the right test immediately.
If you've already been diagnosed, start a symptom diary. Note the time of day, what you were doing, and how long the episode lasted. For those dealing with vestibular migraines, this is the only way to identify the triggers-whether it's a certain food, a crowded mall, or a lack of sleep-that lead to an attack.





Anna BB
18 April, 2026 10:10 AMIt is truly fascinating... how a tiny crystal in the ear can completely shift our perspective of reality... doesn't it make you wonder about the fragile nature of our perception???
Tama Weinman
18 April, 2026 20:08 PMFunny how they push these "maneuvers" and specific diets. I'm sure it's a convenient way to keep us focused on the inner ear while ignoring the frequencies being pumped into the atmosphere that actually disrupt our balance. Just a little tip: if you look into the patents for signal jamming, you'll see why your head is really spinning. But hey, keep following the guidebook if you enjoy being told what to do by "experts".
Maggie Graziano
19 April, 2026 04:57 AMbig pharma loves the water pills
Michael Lewis
20 April, 2026 04:49 AMStop letting the dizziness win! You have to attack these vestibular exercises with everything you've got and stay consistent every single day! I know that first two-week hump feels like a mountain, but you push through it or you stay stuck! Get after it!
Josephine Wyburn
21 April, 2026 08:50 AMOmg you guys I literally cannot even imagine the horror of waking up and feeling the world spin because I already have so much anxiety about my sleep quality and now I'm just lying here thinking about calcium crystals floating in my head like some kind of nightmare movie scene 😱😭 it's just so overwhelming to think that our bodies can just betray us like this without any warning and I'm honestly just spiraling just reading this 😵💫💔
Autumn Bridwell
21 April, 2026 11:12 AMI actually had a cousin who tried the Epley maneuver at home and she ended up practically falling off her bed in a panic because she did it wrong and it was absolutely chaotic! I want to know exactly which therapist she saw because the drama that followed in our family for three weeks was legendary!
Dana Chichirita Nicoleta
21 April, 2026 19:11 PMIt is simply marvelous to know that neuroplasticity allows our brilliant brains to adapt and overcome such challenging sensory deficits through dedicated practice! I am absolutely convinced that anyone who commits to the six-to-eight week program will find their stability returning with a flourish, and it is truly inspiring to see the data supporting such a high success rate for those who persevere through the initial discomfort!
Kim Hyunsoo
22 April, 2026 05:46 AMThe idea of "habituation" is such a trippy concept... basically just boring your brain into submission... (o_o)
Heer Malhotra
23 April, 2026 02:24 AMIt is regrettable that this guide focuses on Western medical standards. India has provided the world with Ayurvedic balance and holistic healing for millennia, which are far superior to these mechanical maneuvers. One must prioritize the ancient wisdom of the East over these sterile, temporary clinical fixes.
Cheryl C
23 April, 2026 21:06 PMUSA all the way baby!! 🇺🇸 we got the best doctors and the best tech to fix these ear things lol!! sry for the spelling but im typing fast 🤪🇺🇸
Richard Moore
24 April, 2026 23:13 PMI totally agree that getting a professional to do the first maneuver is the only way to go! Don't risk messing up your inner ear by playing doctor on YouTube 😡👊 just get to an ENT and get it sorted properly! 👂✨