Opioid-SSRI Interaction Risk Checker
Disclaimer: This tool is for educational purposes only. It is not a substitute for professional medical advice. Always consult your doctor or pharmacist before starting or changing medications.
Select an Opioid Medication:
Interaction Analysis
Reminder: If you experience shivering, rapid heart rate, or muscle twitching, contact emergency services immediately.
Imagine waking up with uncontrollable shivering, a racing heart, and muscle twitches that feel like electric shocks. For some, this isn't a random flu; it's a life-threatening reaction called serotonin syndrome is a serious drug reaction caused by too much serotonin building up in your nervous system, leading to overstimulation of the 5-HT1A and 5-HT2A receptors. It usually happens when two or more medications that increase serotonin are taken together. While it sounds like a rare medical anomaly, millions of people take antidepressants and pain medications every year, making this a very real danger in modern medicine.
The Biological Trigger: How It Actually Happens
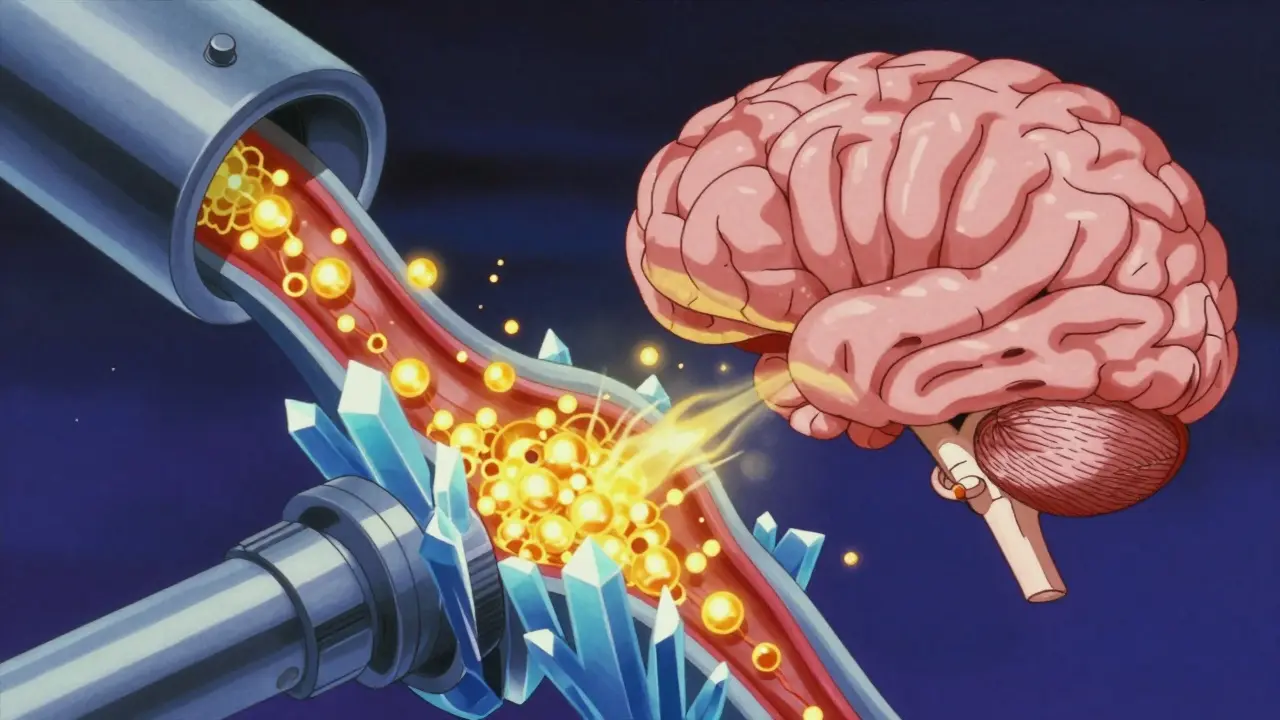
To understand the risk, you first have to understand the serotonin transporter (or SERT), which is the primary protein responsible for vacuuming serotonin out of the synaptic cleft so it can be recycled or broken down. Think of SERT as a biological drain. If the drain is plugged, serotonin floods the area, overstimulating the brain and body.
When you take SSRIs (Selective Serotonin Reuptake Inhibitors), you are essentially plugging that drain to keep more serotonin available to improve mood. Many opioids do the exact same thing. When you combine them, you don't just add the effects-you multiply them. This leads to a toxic surge that can push your body into a state of hyper-excitation.
Not All Opioids Are Created Equal
A common mistake is thinking that any "pain pill" combined with an antidepressant is dangerous. In reality, the risk depends entirely on the specific drug's chemistry. Some opioids have no effect on serotonin, while others are potent inhibitors of SERT.
For instance, tramadol is one of the most problematic opioids because it has a very high affinity for SERT-about 30 times stronger than morphine. Other high-risk options include methadone and pethidine. On the other hand, drugs like morphine, oxycodone, and buprenorphine generally don't mess with serotonin transporters, making them significantly safer alternatives for someone already on an antidepressant.
| Risk Level | Common Medications | Primary Mechanism |
|---|---|---|
| High | Tramadol, Methadone, Pethidine | Potent SERT inhibition |
| Moderate/Variable | Fentanyl | Receptor affinity (5-HT1A/2A) |
| Low | Morphine, Oxycodone, Hydromorphone | Minimal to no SERT interaction |
Spotting the Red Flags
Serotonin syndrome is a clinical diagnosis, meaning there isn't one single blood test to confirm it. Doctors instead use the Hunter criteria to look for specific physical signs. It's not just "feeling anxious"; it's a physical breakdown of coordination and temperature control.
Symptoms usually appear within hours of starting a new med or increasing a dose. They typically fall into three categories:
- Mild: Shivering, diarrhea, and a heart rate over 100 beats per minute.
- Moderate: Muscle twitching (clonus), agitation, heavy sweating (diaphoresis), and tremors.
- Severe: High fever (above 106°F), rigid muscles, seizures, and unconsciousness.
A dangerous trend in emergency rooms is misdiagnosis. About 43% of these cases are initially mistaken for other conditions like neuroleptic malignant syndrome. If you or a loved one exhibit spontaneous ankle clonus (involuntary rhythmic muscle contractions) after taking a new painkiller, it's a medical emergency.
The "Danger Window" and Half-Lives
You might think you're safe if you stopped taking your antidepressant a few days before starting an opioid, but that's not always true. The risk depends on the drug's half-life-the time it takes for the concentration of the drug in your body to reduce by half.
Take fluoxetine. Its active metabolite, norfluoxetine, can stay in your system for up to 16 days. This creates a massive "danger window." If you switch from fluoxetine to a high-risk opioid too quickly, you can still trigger serotonin syndrome even though you aren't actively taking the pill. In contrast, sertraline has a much shorter half-life (about 26 hours), meaning the risk clears faster.

Prevention and Safety Strategies
The best way to prevent this reaction is to avoid high-risk combinations altogether. If you are on an SSRI, ask your doctor if a lower-risk opioid like morphine or oxycodone is appropriate for your pain. If a high-risk drug like tramadol is absolutely necessary, some pharmacists recommend starting with 50% of the standard dose and monitoring the body closely for the first 72 hours.
For those switching medications, a "washout period" is essential. While 14 days is standard for many antidepressants, experts suggest waiting up to 5 weeks after stopping fluoxetine before starting another serotonergic agent. For older adults, the risk is even higher because the liver and kidneys don't process drugs as efficiently, which can lead to toxic buildup even at normal doses.
What to Do in an Emergency
If serotonin syndrome is suspected, the first step is the immediate stop of all serotonergic drugs. This isn't a "taper off" situation; it's an immediate cessation. In severe cases, hospitals use cyproheptadine, which is a medication that blocks 5-HT2A receptors to stop the serotonin overload. Supportive care, such as benzodiazepines for agitation and cooling blankets for high fever, is critical to preventing organ failure.
Can I take Tylenol or Advil instead?
Yes. Acetaminophen (Tylenol) and NSAIDs (Advil/Aleve) do not affect serotonin levels and do not carry the risk of serotonin syndrome when taken with SSRIs.
Is tramadol always dangerous with antidepressants?
It's not "always" dangerous, but it's high-risk. Many people take them together under strict medical supervision, but because tramadol inhibits SERT, the chance of a reaction is significantly higher than with other opioids.
What are the first signs I should look for?
Watch for unusual shivering, rapid heart rate, and muscle twitching-especially in the ankles or eyes-accompanied by sudden agitation or sweating.
Does fentanyl cause serotonin syndrome?
While lab tests show fentanyl doesn't block the serotonin transporter (SERT), there are over 100 clinical case reports of people developing serotonin syndrome from it, likely due to its effect on serotonin receptors.
Are there genetic factors that make me more susceptible?
Yes. People who are "poor metabolizers" of the enzyme CYP2D6 have a significantly higher risk (about 3.2 times higher) because their bodies can't break down these drugs efficiently.




Ajinkya Joshi
22 April, 2026 16:31 PMOh wow, a guide on how not to accidentally kill yourself with common meds. Truly groundbreaking stuff that definitely isn't already in the pamphlet the pharmacist hands you. I'm sure the 43% of doctors who misdiagnose this are just waiting for a Reddit post to teach them how to do their jobs properly.
Olayinka Ibukunoluwa Mercy
23 April, 2026 19:16 PMThis is such an important reminder for all of us!!! ❤️ Please, please always double check with your healthcare provider before starting anything new!!!! Your health is your wealth!!! ✨🙏
Chidi Prosper
24 April, 2026 09:18 AMExactly. The point is that patient advocacy is the only way to avoid these mistakes. If the doctor doesn't know your full med list, the fault lies with the system, but the consequence is on the patient. We need to be assertive about our drug interactions.
RAJESH MARAVI
24 April, 2026 17:38 PMwow so we just trust the "doctors" now?? lol. probbaly just a way to push more expensiv meds on us while the cheap ones "cause synderome"... totaly sus
Sarah Watters
26 April, 2026 16:57 PMIt's funny how these "risk levels" always seem to align with whatever the big pharmaceutical companies are pushing this quarter. The way they categorize some drugs as low risk is just a convenient way to keep the profit margins high while keeping the population sedated and compliant. Just typical institutional gaslighting.
Divyanshu Giri
27 April, 2026 17:44 PMKeep your head up everyone! Just stay sharp and talk to your doc to keep the vibes high and the body healthy! You got this!
Dan Wizard
28 April, 2026 09:26 AMI find it quite fascinating how the biological mechanism of the serotonin transporter operates almost like a complex plumbing system, and it really makes me wonder if there are other unexpected interactions with common over-the-counter supplements that we aren't being told about, especially since some herbal remedies also affect serotonin levels in ways that aren't as widely documented in these standard medical summaries.
Rick Brewster
29 April, 2026 17:31 PMthe sheer banality of the human condition is mirrored in the chemical fragility of our synpatic clefts where a mere molecular misstep leads to systemic colapse... its almost poetic how we try to engineer hapiness with SSRIs only to risk a total somatic rebellion because we forgot to account for the half life of a metabolite... truly we are but ghosts in a very leaky machine
Ally Warren
1 May, 2026 12:17 PMIt really puts into perspective how precarious the balance of our mental state is. We spend our lives trying to tune the instrument of the mind, only to find that the strings can snap if we play too many notes at once. The danger window of fluoxetine is a metaphor for how the past always lingers in our biology, refusing to let go even when we think we've moved on to something new.
Odicha ude Somtochukwu
3 May, 2026 06:35 AMIt is indeed imperative that we maintain a high standard of vigilance regarding pharmaceutical interactions!!! The detailed breakdown provided here is most beneficial for the community, and I strongly encourage everyone to maintain an updated list of their current prescriptions for their providers!!!